

I have a confession… I like coffee.
I like coffee in the morning.
I like coffee in the afternoon.
I like coffee black. I like it white.
I like it with sugar, with chocolate, or just plain.
I like the taste of coffee.
I like the way it makes me feel and helps me stay focused.
getting more out of my coffee
Do you know how I could enjoy coffee more?
I could stop drinking so darn much of it, that’s how.
If I drank less coffee I would restore my sensitivity to it.
It would then give me more of a hit when I did occasionally have it.
getting less out of my insulin
In a similar way that many of us have become addicted to coffee that leaves us less sensitive to the impact of caffeine, many of us have also become addicted to cheap processed simple carbohydrates that leave us insensitive to insulin. We become more sensitive to carbohydrate and insulin if we have less of it.
the physiological insulin resistance straw man argument
One of the criticisms that is levelled at low carbohydrate diets is that it causes what is called ‘physiological insulin resistance’.
This can mean that a person who is restricting carbohydrates may end up with higher fasting blood sugars and may have higher blood sugars after a higher carbohydrate meal.
Check out this video to see how some interpret ‘physiological insulin resistance’ to be a bad thing and a reason to eat lots of carbohydrates.
diabetes diagnosis criteria
There are a number of factors that are considered in the diagnosis of someone with type 2 diabetes: [1]
- HbA1c, which is a measure of your average glucose over the past three months,
- random blood sugar,
- fasting blood sugar, and
- oral glucose test.
what is physiological insulin resistance?
One of the clearest explanations of physiological insulin resistance I’ve seen comes from Paul Jaminet who says that physiological insulin resistance is a protective response of the body that ensures that the brain gets the benefit of a limited supply of glucose.
Because the rest of the body is refusing to take up glucose, and the liver takes it up slowly, a meal of carbohydrates is followed by higher blood glucose levels in someone on a low carbohydrate diet.
The human body is very adaptive to different situations and different fuel sources. Just because our reference data is from the past few decades when we have typically eaten large amounts of processed carbohydrates, we take that as the new normal.
Is physiological insulin resistance such a bad thing?
Maybe, maybe not.
Let’s look at what this means when it comes to the various tests that are done to diagnose diabetes.
oral glucose tolerance test
Yes, you may fail an oral glucose test if you are on a low carbohydrate diet due to physiological insulin resistance. But this guy will probably see a rise in his blood sugars too if you fed him the equivalent of two cans of Coke in one hit. [2]

If you have a large dose of fast digesting carbohydrates your body is not primed to dump a pile of insulin into the system. It takes a while to wind up and adjust to large amount of carbohydrates. You also don’t have a high level of insulin washing around in your system from the last pizza meal.
It’s sort of like me and my coffee addiction. Because there is not a lot of time when I don’t have some caffeine in my system I am not as sensitive to caffeine as I would be if I only had an occasional cup.
If you do want to pass an OGTT all you have to do is increase your carbohydrates for a few days before the test and your pancreas will increase the amount of insulin in your system and be better prepared for a high dose of carbohydrates. [3]
fasting blood sugar
Some people may find that their fasting blood sugars rise a little when they start consuming more fat and decrease carbohydrates, particularly if they increase their fat intake.
This is an area where your mileage may vary. I have seen some people run at very low carbohydrate levels and end up with progressively higher fasting blood sugars. Others see their fasting blood sugars continue to come down and ketones go up as they decrease the insulin load of their diet.
When on a lower carbohydrate diet you won’t have high levels of insulin floating around in your system and your body may choose to run blood glucose levels a little bit higher by secreting more glucose from the liver. This is not really a problem if you feel OK.
Many people find this to be a passing phase and after a time of keeping the insulin load of their diet low see their blood sugars come down.
As you keep the glucose load of your diet low you will ‘dry up the root’ and eventually after glucose stores in the liver are depleted, your fatty liver is resolved and your body fat levels are reduced you just won’t have as much glucose available for your liver to keep pumping into your bloodstream.

If you find that you don’t feel good at very low carbohydrate levels then by all means increase your carbohydrates and protein particularly to ensure that you are getting adequate nutrition. Check out the Goldilocks glucose zone article for more thoughts on how to find the right level of glucose for you.
Most people find that their calorie intake decreases with a LCHF approach, however as this study from Dr Thomas Syfriend shows long term excess calories even with a high fat diet is probably not going to end well. Intermittent fasting or tracking your calories to make sure you’re not overdoing the butter may be helpful if you’re not achieving normal fasting blood sugars.
random blood sugar
Carbohydrates are the most potent thing that raises blood sugar. If you are on a low carbohydrate diet chances are your random blood sugar (i.e. non-fasting) will be much lower than if you were on a high carbohydrate diet.
With a smaller amount of dietary carbohydrates you should see much lower post meal blood sugars.
Generally the small amount of insulin that you generate after meals will bring your blood sugar down quickly.
HbA1c
With lower post meal blood sugars your average blood sugar will likely be much lower on a low carbohydrate diet. Therefore your HbA1c, which is a measure of your average blood sugar over three months, [4] should be lower.
insulin levels
We are now understanding more and more that insulin resistance is public health enemy number one. Insulin resistance is a better predictor of heart disease than HDL, LDL, BMI and smoking! [5]
Making sure you have some time when high levels of insulin are not floating around in your bloodstream will help increase your insulin sensitivity and enable your body to manage your blood sugars.
Consistently high levels of carbohydrates will ensure that your insulin resistance stays high!
I am probably not going to stop drinking coffee any time soon, but in view of the evidence, I do try to make sure that I have periods where I give my body a chance to restore its sensitivity to insulin!
If you are interested in reducing your insulin load while ensuring that you achieve great nutrition that supports your goals, check out this list of optimal foods and meals.
Keep Reading
- What Does Insulin Do in Your Body?
- How to really reverse your insulin resistance
- How to reverse type 2 diabetes and optimise your blood sugar
- Macros Masterclass
- Data-Driven Fasting: How to Lose Weight and Reverse Type 2 Diabetes Without Tracking Food
- Turning the Tide on Type 2 Diabetes: Real Stories of Reversal
Marty this was a very interesting post! I’m definitely going to look more into physiological insulin resistance, I didn’t even know this was a thing.
Also, I won’t spam your comments section about it, but I might have something you might be interested in re: blood-sugar controlling coffee. If so, let me know 🙂 thanks for the great post!
Thanks Sarah. I would be interested in your other inputs on blood glucose and coffee. I think it probably largely depends on what you put with the coffee (e.g. milk, cream, sugar, mct oil, butter). Using coffee to burn yourself into the ground is probably also not great for overall health and blood sugar control either.
I have not noticed the slow increase in Blood Sugar from the Coffee, not that is is guaranteed for everyone, but any idea as to what timeframe were looking at for this to occur (if it does occur)? Glucose at 88 and holding.
Mark
Mark
I think you’d just see a blood glucose rise due to an additives in the coffee rather than the coffee itself which has minimal calories.
Major coffee abuse, a lack of sleep and general exhaustion may cause insulin resistance, but it’s not necessarily related to the coffee.
In the article above I was just trying to draw the parrallel beteween caffiene resistance and insulin resistance to make the point that increasing carbs is not a logical way to improve insulin resistance.
Cheers
Marty
Very true Marty. Coffee: the double-edged sword! We feel like we can’t live without it sometimes and then others, we drink too much and feel queasy and horrid for hours. Before diabetes I used to looooove lots of cream and sugar in my coffee– I still like it to be not bitter so I currently use just a teaspoon of half and half and the same of stevia. Seems to have no significant affect on my blood sugar according to my meter. I actually found out recently about a blood sugar-controlling green tea and I’ve been really liking it– the company also offers a weight-loss coffee but that particular product isn’t one that I need at this point as I’m trying to maintain a more stable weight after a recent DKA experience. But anyway, I just wanted to share the fact that there is a product tea/coffee product out with health benefits + your daily pick-me-up 🙂
Hello. I am new to your blog. What I see so far is very helpful. I have a feeling this will be a great source of information. Thanks for sharing your knowledge.
Thanks Will. Glad you’re enjoying it!
I was wondering what the mechanism or pathway is for dietary protein to raise insulin. With carbs, it’s pretty easily explained by the blood glucose rise and resulting increase in insulin to clear it. But what makes dietary protein insulinogenic? I mean the pathway, or the mechanism. Any thoughts on this? TIA.
Hi Wendy
Amino acids from digested protein are either glucgenic, ketognic or can be both. See http://en.wikipedia.org/wiki/Glucogenic_amino_acid for a high level summary.
I have another post coming out on 6 July 2015 on that goes way too far down the rabbit hole on the topic.
The energy from protein not required for muscle growth and repair (i.e. protein synthesis) doesn’t magically disapear. The aminos will circulate in the blood stream until they are required for energy, with the glucogenic aminos being turned into glucose to be uses as if they were carbs.
These glucogenic amino acids then require insulin to be metabolised or stored as fat as if they were carbs.
Cheers
Marty
Marty,
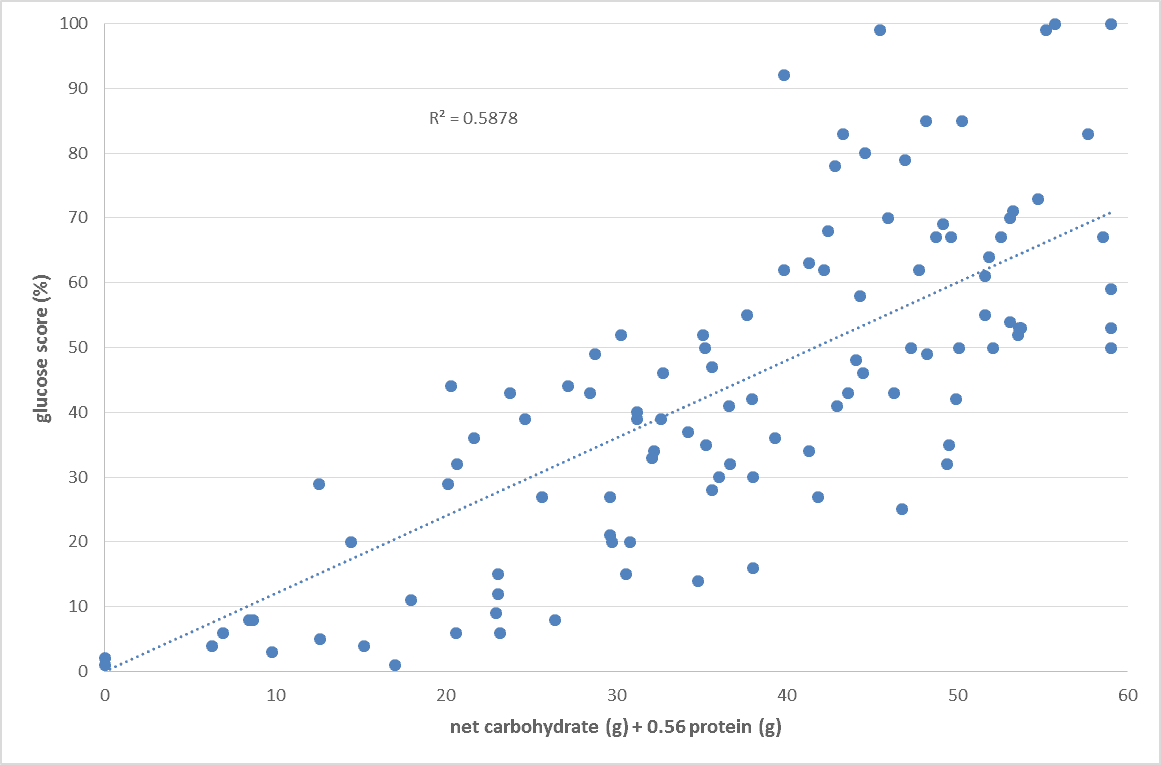
Check me on this, but “Glucongenesis” is what it’s called. 58% of the Protein (seems very specific, but that’s what I remember reading) ingested is converted into Carbohydrates. This is why Low Carb eaters can never really eat too few carbs….you simply convert Protein to Sugar.
Mark
That’s pretty much it Mark.
The 56% is based on statistical analysis of a bunch of datapoints in real life people with real life foods. In reality this depends on a lot of factors like how much you’re eating and how active you are, but that seems to be a pretty useful factor that can help us calculate and compare the insulinogenic ratio of various foods.
Check out this article https://optimisingnutrition.wordpress.com/2015/06/04/the-goldilocks-glucose-zone/ on how you can consider your glucose : fat ratio rather than protein : carb : fat ratios.
Cheers
Marty
Hi Marty – thank you for your reply. The answer gives me another question, and that is, what is the mechanism by which these “excess” amino acids become ketogenic or glucogenic. My understanding is that gluconeogenesis is triggered/controlled by glucagon, so perhaps that is the answer for the extent to which gluconeogenesis occurs with these glucogenic amino acids. Is there another pathway it mechanism for gluconeogenesis that you know of? And, what pathway or mechanism controls the ketogenic amino acids bring turned into ketones? If you know? I hope these questions/discussions aren’t a bother. TIA.
I like your questions.
It seems that to some degree the glucose / ketone split is already somewhat predetermined. http://en.m.wikipedia.org/wiki/Glucogenic_amino_acid
See also http://en.m.wikipedia.org/wiki/Gluconeogenesis
The body requires about 7% of calories from protein for muscle growth and repair. I think perhaps the body will cover this with glucagon with mutes the glucose rise. With higher levels of protein the body doesn’t negate the insulinogenic effect with glucagon in the same way.
I have a couple more post in the wings that discuss this in more detail.
I don’t have all the answers, just some question to get the discussion going.
Interesting. I note the wiki says these AA’s “can be” (not “are”) converted to glucose, so I personally am not so sure their fate as glucose is predetermined – again, glucagon is the control, it seems, that turns on the switch to convert these AA’s to glucose when/as needed. I’m also interested in the “switch” or pathway for ketones. I’ll have to explore that further and of course will be glad to share what I find.
Can I ask your source for the 7% protein figure? I (non-diabetic) rely on Volek & Phinney’s estimation, which is not a straight % (esp as energy intake is highly variable) but is a bare-bones minimum based on your size (of lean mass, 1 g/kg) and goes up from that minimum number based on activity level, whether you’re healing or aging, aiming to increase lean mass, etc. I am not trying to challenge you at all, I hope I do not come across that way, I am just trying to nail down all the mechanistic details for my own understanding, and you are obviously a well-informed source. Thanks for taking the time to respond.
See minimum protein requirement section inhttps://optimisingnutrition.wordpress.com/2015/06/04/the-goldilocks-glucose-zone/# which emerges to http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3636610/
Thanks. Just wanted to note that this protein level is merely cited in this study, it’s not a finding, and in fact is pulled from the Dietary Reference Intakes created by the USDA. These in turn are based on each person’s size, and are stated in the DRI as being a minimum amount to avoid chronic disease, not the amount needed for optimal health. Protein beyond that needed for “optimal health” is surely “excess,” but not the amount between “avoid disease” and “optimal health” levels, which is a grey zone and surely individual. Also, since this number comes from the USDA, it bears mentioning that the USDA has had a historic problem with lacking scientific bases for their recommendations, rendering these particular recommendations questionable as to credibility also.
There’s a big fear of “too much protein”/GNG in the LC world, and I’m trying to track down what the real, scientific basis to that is (if any). That’s the reason for my interest.
Have you seen this article?
I don’t think it’s a matter of too much protein or gng. It’s just a matter of balancing that with your own pancreas’ ability to keep up with the glucose load.
If you can go nuts on carbs and protein and your blood sugars are excellent then good luck to you. I’m envious! See https://optimisingnutrition.wordpress.com/2015/03/22/diabetes-102/
I can’t! But I do well on 100-120 g protein, while LC. I am tryin to drill down on the basis for the protein phobia. As you say pancreas load is the issue, but again that’s only as to excess so defining that become critical. Also – was there a missing link for an article in your last comment? All best.
You also need to make sure you get adequate amino acids, so although 7% may be adequate for 50% of the population something like 15 to 20% is often optimal to get aminos for the brain and everything else.
Here’s the link with some thoughts on optimal blood sugars and why they are important.
https://optimisingnutrition.wordpress.com/2015/03/22/diabetes-102/
I’ve read that, it’s a(another) great article. I have done some monitoring of BG (results 80s-90s, even post-prandial, thank you LC diet), and have a good hba1c (but also know if the decreased reliability of that test in healthy people, with RBC tending to live longer, absorb more glucose over that longer life, and this possibly giving a falsely high value). I think for us non-diabetics it’s a waste to continually re-check BG; periodic spot checking seems more than adequate, don’t you think?
Thanks Wendy
My wife who is type 1 does blood sugars say five times a day.
I was doing a couple a day for a while when I was trying to troubleshoot my diet and fasting. I have stopped checking now that I have reached where I wanted to be. I plant to check occasionally similar to the way that I’d check my weight occasionally and tighten things if I’m not making the progress I want to.
Agree that if your blood sugars and HbA1c are fine then no need to check regularly, though there is a lot to be learned by testing when you’re not getting the results you want.
Similar thing for food tracking. It’s no way to live over the long term, but you can learn a lot by tracking and reviewing for a while.
Cheers
Marty
I see you’re doing the OKL macros. I have a lot of respect for Raymund! Where do they end up sit in on the chart. Are the highly ketogenic or is there higher protein? https://optimisingnutrition.wordpress.com/2015/06/04/the-goldilocks-glucose-zone/
More ketogenic (though perhaps you disagree?) with 109 g protein recommended, 27 net carbs max. This is lower, though, than what Phinney actually shows in his “Four Phases” pic (in the video on the linked post). If you calculate each element, Phase 1, Adapt, actually includes 140 g protein and 35 g carbs, for a total insulin load of 175 g. Each phase decreases protein by 10 g, but the initial two phases ADD 10 g carbs, thus the insulin load stays 175 for all of the losing. This is above your Goldilocks zone. Do you think Phinney’s numbers are too high? Hasn’t he used those to run weight loss studies?
What’s that in terms of macro percentages that you’re eating? I would be interested to see where it sits on the carbs / protein chart which is an adaption of Phinney’s WFKD chart.
An insulin load of 175g still seems pretty high. I would think if you were to drop the protein to get more into the ketogenic zone you would then just eat fat to satiety (not excess).
I would be interested to see some daily food diaries if you have them. I’m interested in running some analysis ideas to see if the system is helpful to tweak and refine.
Are you part of this FB group? I was hoping to run a few worked examples through the system to help develop and refine and get some feedback. It would be great to have your involvemnet. https://www.facebook.com/groups/optimisingnutrition/
I’m not eating 175 g, those are *Phinney’s* numbers, if you calculate each of the Four Phases. I’m wondering the source for you saying that Phinney says 150 g is the ketogenic threshold? I don’t understand why he uses different number in the Four Phases chart, which never goes down to 150 (Phase 4 is still 165, 55 carbs and 110 protein). Yes, I am in your FB group. How would I share a sample food diary? I am not sure I want to publicly share something like that on FB, where anyone and everyone I know on FB could potentially see it. How does sharing the diary work?
I like your questions!
The 150g is a conversion of Jaminet’s 600g of carbohydrates to glucose from carbs or protein.
I think the border of Phinney’s WFKD triangle represents approx 500 glucose calories or 125g of glucose.
I just ran the numbers on Phinney’s four phases chart and I get a glucose load of 55g for the adapt phaes, 71g for adjust, 84g for build and 86g for maintain.
The FB group is closed so it’s only viewable for people in the group (220 ppl). You could send me the MFP diaries via FB messenger and I could run the numbers and do up a .doc and send it to you to make sure it makes sense before I shared it with the group for feedback and a learning experience.
I’m intrigued with the idea of balancing amino and vitamins and would like some real life examples to work through to get some feedback.
? I don’t follow. Protein levels alone are a higher insulin load than this under your “insulin load” formula; they are 140 g, 130, 120 and 110 in each of the phases. Phase 1 = 140 * 0.56 = 78.4 from protein alone. Am I missing something? Also, for carbs, what are you assuming are fiber?
Wait, I’ve figured out what I’ve missed, you’re subtracting an amount for “actual protein needs ” or perhaps 10% of tdee, then calculating the load from the excess protein beyond that figure?
Yup. It’s a bit convoluted but it works.
The body doesn’t behave according to Excel formulas but I think it’s useful.
how many days’ worth of food diaries are you interested in?
Somewhere between one and five.
I’ll send 3 days (right down the middle). I can only create the report in PDF, I hope this works. If not, would you please point me to guidance to create a .doc
Have a look at section 10.16 of the updated manifesto… I’ve run some worked examples as far as the glucose load goes comparing it to Phinney’s four phases.
See https://www.dropbox.com/s/ninuwyreda0epix/Optimising%20nutrition%2C%20managing%20insulin.docx?dl=0
Hi marty,
I what to take the opportunity to say thank you for the time you have invested in creating such an educational resource. 2nd to none and I’ve spent a fair amount of time reading Dr Attia’s and many others as well. Well done!
I have a few questions if you don’t mind providing your thoughts. A little of my history to set up my question. -( Im 6’2” 180lbs/10%BF)when i originally started LCHF, approximately 6 months ago (60-70 gross carbs/ fat approx. 220g), my glucose levels feel from a fasting state of 104 mg/dl to 93 in the first 2 or 3 months,great right… then my fasting glucose started to rise and ended up at 118 mg/dl. I immediately thought I must be adding more fat to my already fatty liver and asked my Doc for metformin to keep me from full blown T2 and give me time to work on this. At that point I started intermittent fasting 18/6 which put me into ketosis most of the time and my fasting and daily glucose levels were optimal. I since reduced my carbs to net about 25 or 30g/day because everytime I eat my ketone level drops below .5 mmol for 2 or 3 hours taking me out of ketosis. Now that I have dropped my carb intake again my fasting glucose level rose again to about 118 mg/dl. I started researching on your site for information and found Physiological Insulin Resistance. This could very well apply to me? Very frustrating, everytime I make an adjustment thinking I’ve dialed it in, a new challenge arises. Hoping yo help me with some direction, Im not sure which way to proceed.
1st question – Should ones ketone level always stay above .5mmol to be considered ketonic even following a meal?
2nd – thoughts on Physiological IR applying in my case and just your over all thoughts please.