

Cancer affects not only one’s physical health but also tests the endurance of their spirit. Amidst the medical consultations and treatments lies a significant yet underexplored realm of healing: nutrition.
This article unveils a collaborative endeavour where experts have curated a series of nutrient-dense foods and recipes specifically for cancer patients. This initiative aims to bridge the gap between theoretical nutritional advice and practical dietary solutions, allowing cancer patients to embark on a journey of nutritional optimization amidst their fight against cancer.
Delve into this read to understand the synergy between nutrition and cancer management and how you can harness the power of a tailored diet in your battle against cancer.
- Who is Brian Lawenda?
- Why did we create three recipe books for cancer?
- This is not magic!
- The diet to prevent cancer is not the same as when you have cancer
- What is cancer?
- We all have some cancer cells
- Obesity
- Nutrient-dense recipes for fat loss and insulin resistance
- Cancer is opportunistic
- Carbohydrates
- Hormones
- Fat and ketones
- Should you go ‘plant-based’ or ‘vegan’ to manage cancer?
- Nutrients that affect cancer growth
- Nutrient density and cancer
- Do you still need to use supplements?
- What about the various cancer phenotypes?
- Weight gain
- Weight maintenance
- Summary
- The recipe books
- Learn more
Who is Brian Lawenda?
Dr Brian Lawenda MD has a unique background as:
- a radiation oncologist,
- an integrative oncologist, and
- a functional medicine practitioner.
Brian is the National Director of Integrative Oncology and Cancer Survivorship, GenesisCare and brings a wealth of knowledge and practical experience to this discussion.

Brian has been a close friend to Optimising Nutrition for years and there is a lot of alignment in our approaches. When we started thinking about who we could ask to be on our board of advisors, Dr Lawenda was an obvious choice for us to partner with (along with Dr Ted Naiman, Diana Rodgers and Bev Postma). We have also been working with Brian to develop an automated approach to fine-tuning nutrition for his cancer patients.
Why did we create three recipe books for cancer?
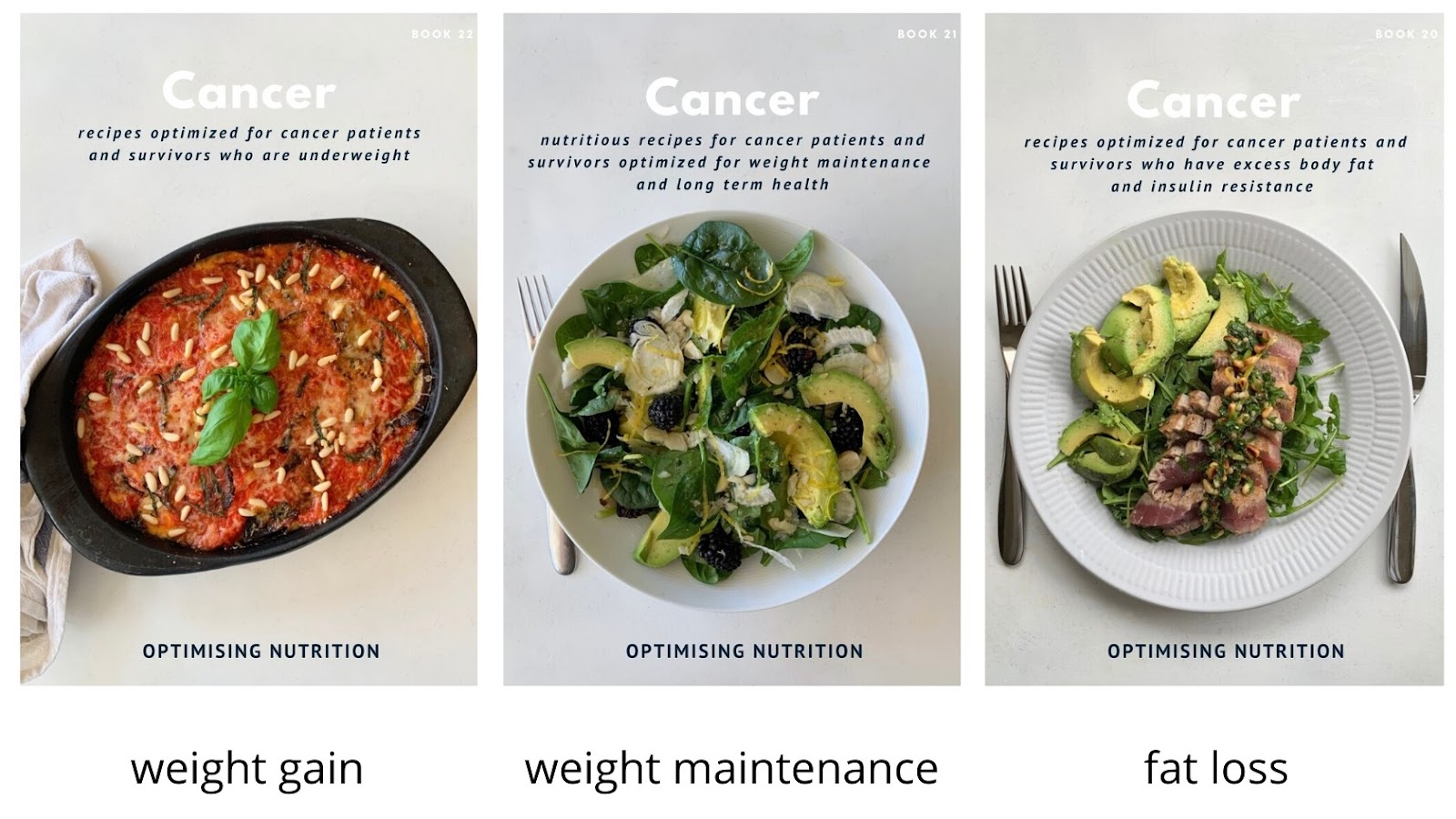
When we first talked about building recipe books tailored for people managing cancer, Brian insisted there wasn’t a one size fits all solution.
- Weight gain
- Many people managing cancer lose their appetite during the aggressive treatment regime (e.g. radiation and chemotherapy) and need to find a way to eat more to put weight back on and avoid sarcopenia.
- Fat loss
- Meanwhile, many people need to lose weight before cancer treatment. Obesity is a significant risk factor for cancer growth.
- Maintenance
- People who are already at a healthy weight simply need to focus on nutrient density while getting enough energy to maintain their weight.
“There is no one ‘anticancer diet.’ Whether you are going through cancer treatment or you are a cancer survivor, your diet needs to support your metabolic health, immunity and gut health. To effectively fight cancer, tolerate treatment and recover, your body requires a nutrient-dense diet that is tailored to your needs.”
Dr Brian Lawenda

This is not magic!
What we have created is not magic.
Our nutrient-dense recipes for people managing cancer are simply packed with minimally processed ingredients tailored to suit the needs of people managing cancer.
There is still a role for targeted drugs and other therapies in the effective treatment of cancer under the guidance of your medical team.
Our recipes are designed to give your body what it needs to recover and thrive (as much as possible) through the process of cancer management while minimising the nutrients that promote cancer growth.
In addition to medical intervention, we believe that lifestyle and dietary changes will give you a MUCH better chance of long term success.
The diet to prevent cancer is not the same as when you have cancer
I was chatting recently with long term cancer survivor and author of How to Starve Cancer, Jane McLelland. She was adamant that the diet to prevent cancer should be very different from your diet when you find you have cancer.
We created the cancer recipe books only after we built a series of 19 other books designed for people that do not have cancer. However, once you have a cancer diagnosis, your focus needs to change.
What is cancer?
At the simplest level, cancer can be thought of as excessive growth of defective (or malignant) cells.
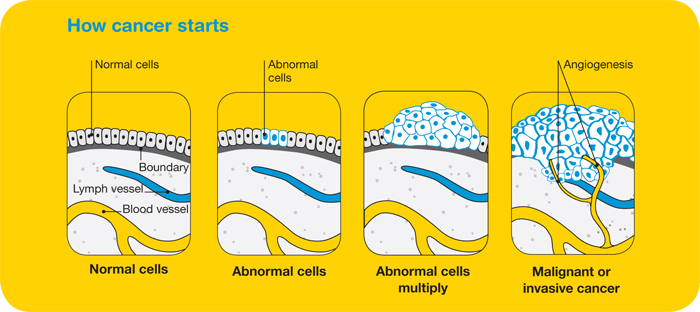
We usually want to support healthy growth and repair (e.g. in the context of growing children or people who are building muscle). However, someone managing cancer needs to restrict the growth of cancer.
We need to starve malignant cells while also nourishing the person who has cancer (the host) at the same time.
To achieve this, we need to find the optimal balance tailored to a person’s goals and context by reducing the nutrients that promote cancer growth while still giving their body the energy and nutrients it needs to recover, heal and thrive.
We all have some cancer cells
Everyone has pre-malignant cancer cells.
In healthy people, these defective cells are cleaned up regularly before they become a problem. A healthy balance of feeding and fasting enables both growth and repair to occur. However, in a person who develops cancer, for a range of reasons, this repair cycle becomes unbalanced.
While many people with cancer find benefit in fasting, going without food for an extended period can be challenging for people undergoing cancer treatment. Eventually, you need to eat something. If you chose to incorporate fasting into your cancer treatment regime, your choice of food when you do eat becomes even more critical.
Obesity
As with many things related to health and longevity, obesity is a key risk factor for cancer.
When we provide a stream of poor quality fuel, we set up an environment of growth (anabolism) with less time for repair, breaking down (catabolism) and cleaning (autophagy).
As shown in the chart below, the relative risk of a range of cancers increases with increasing Body Mass Index (from Quantitative association between body mass index and the risk of cancer: A global Meta-analysis of prospective cohort studies: Obesity and cancer risk).
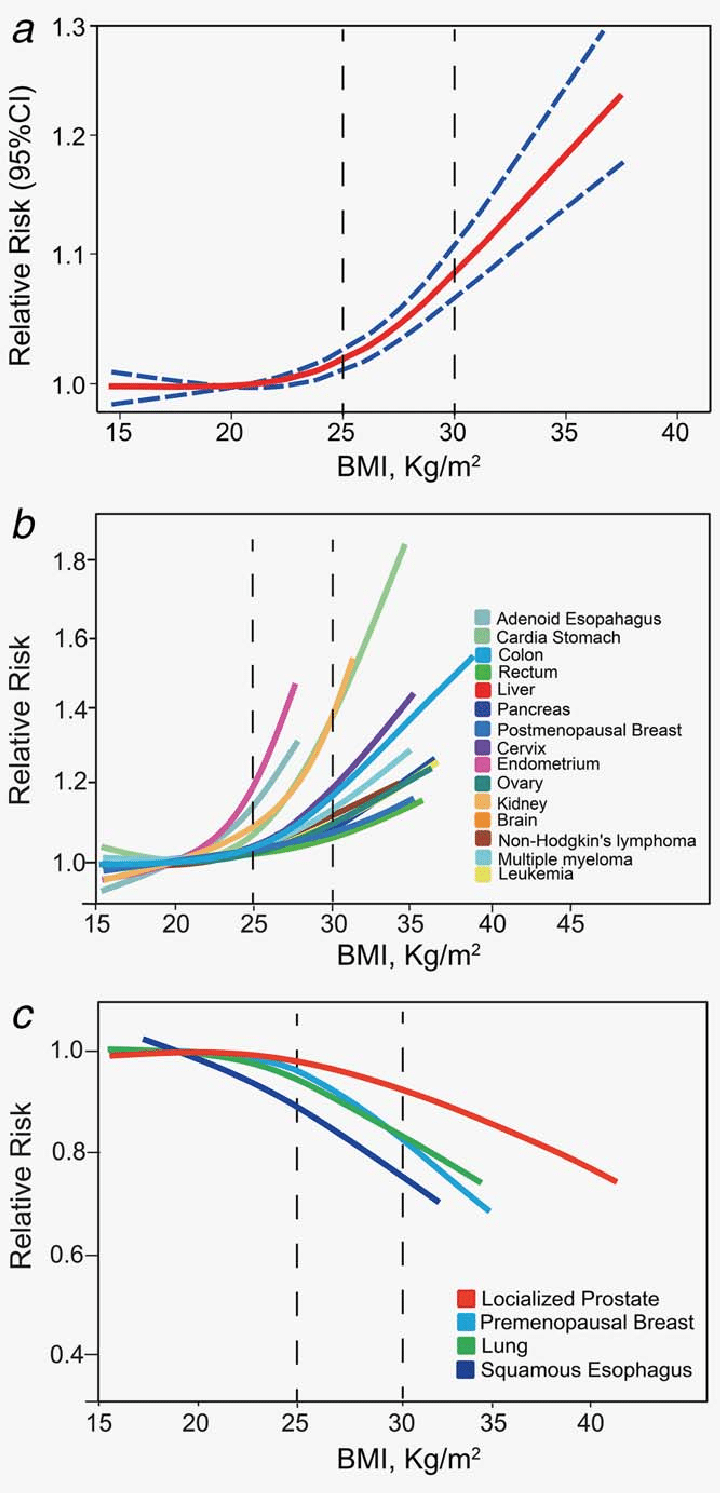
Having excessive body fat causes systemic inflammation, insulin resistance, immune suppression, impaired DNA repair and increased production of free radicals, cancer growth factors and estrogen. Each of these contributes to a cancer-promoting environment in our body.
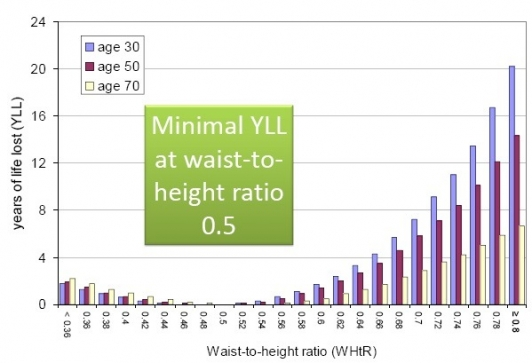
If you have cancer and are overweight (i.e. you have a waist to height ratio of greater than 0.5), one of the best things you can do is to reduce your body fat.
Nutrient-dense recipes for fat loss and insulin resistance
This is the reason we created a book of recipes tailored for people with excessive body fat to help manage insulin resistance.
The recipes in this book focus on maximising nutrient density and satiety while providing less of the nutrients that are believed to fuel cancer growth.
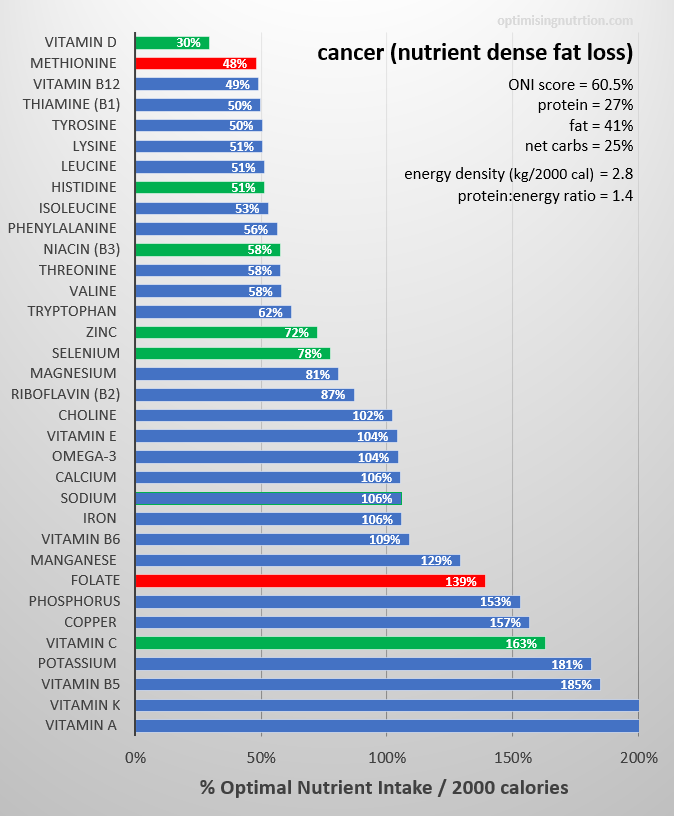
The micronutrient fingerprint chart below is from our fat loss and nutrient density cancer book. It shows the nutrients that these recipes contain as a percentage of the Optimal Nutrient Intake. The red bars show the nutrients that have been de-emphasised (i.e. methionine and folate), while the green bars show the nutrients that have been prioritised.
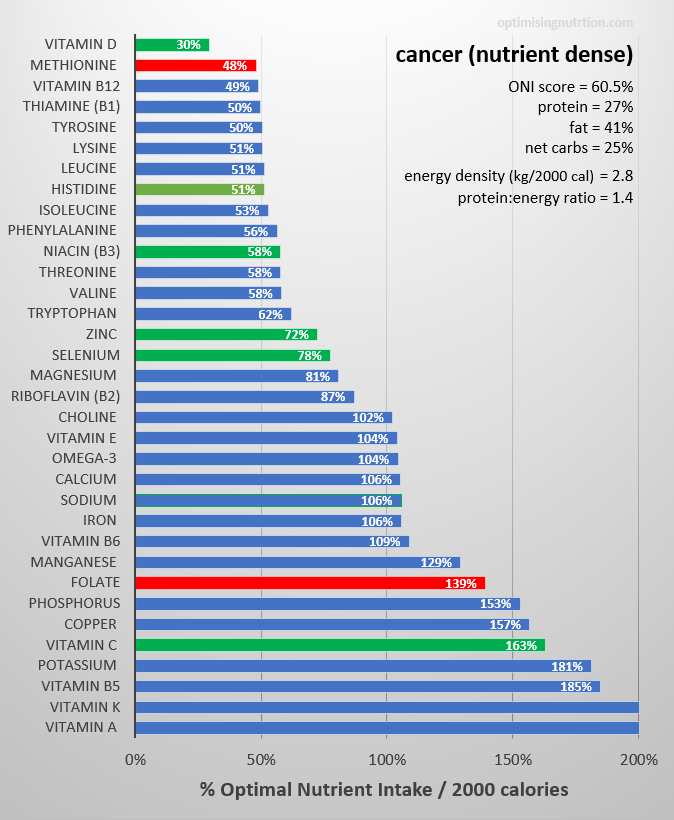
They provide a very high level of most of the essential nutrients on a calorie for calorie basis. They will increase your satiety to help you feel fuller for longer with fewer nutrient cravings, which will lead to weight loss.
Some photos of the highest-ranking nutrient-dense recipes tailored for cancer are shown below.




Cancer is opportunistic
Cancer is highly opportunistic. This means that it will adapt to its environment to feed on any fuel it can get access to (i.e. carbohydrate, protein, fat and even ketones).
While we can decrease the availability of the nutrients that tend to fuel cancer the most, you need to be aware that cancer can adapt and change fuel sources.
For example, if you limit protein, your body will break down muscle (which can lead to sarcopenia) and release amino acids that can fuel cancer growth.
In more advanced stages of the disease, called “cachexia”, cancer forces your body to give up lean muscle tissue to feed it.
Carbohydrates
But of all the nutrients, It appears that cancer loves to feed on simple carbohydrates the most. Hence, reducing the glucose in your diet is one mechanism to starve cancer cells while still fueling the rest of your body.
While every cell in your body uses glucose, cancer cells use about 200 times as much as healthy cells. Many types of cancer cells have more insulin receptors than healthy cells, making them respond to anything that increases insulin. Glucose feeds several anabolic processes that are enhanced in cancer cells and are vital for their proliferation.
Research stemming from the work of Nobel Prize Winner Otto Warburg in 1918 suggests that cancer cells feed heavily on glucose through aerobic fermentation which drives cancer cell growth more than other substrates (e.g. fat and protein). Cancer cells tend to favour glycolysis rather than oxidative phosphorylation (which is preferred by most of the other cells in the body).
Keeping your blood glucose levels lower will reduce cancer’s access to glucose, which has been shown to slow tumour progression and improve cancer outcomes. By contrast, our modern processed diet contains plentiful refined carbohydrates.
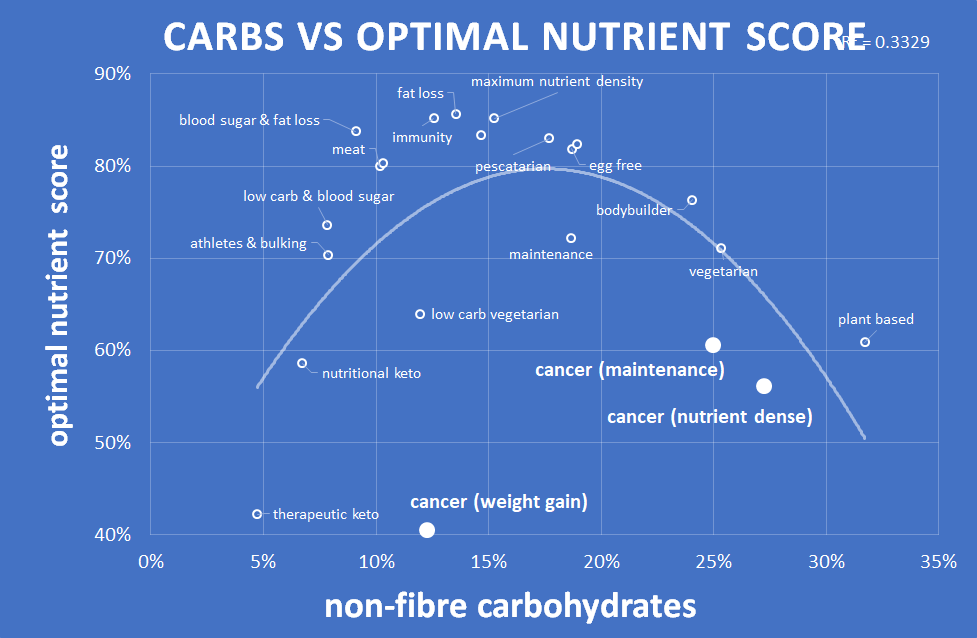
While the Warburg Effect is still controversial today, all our nutrient-dense recipes tend to be lower in non-fibre carbohydrates, which will help reduce the easy fueling of cancer cell growth.
The chart below from our analysis of our series of 22 recipe books, shows that we tend to see optimal nutrient density at around 15 – 20% non-fibre carbohydrates in our diet.
Hormones
An environment that supports high levels of growth also corresponds to higher cancer growth. Some of the hormones that correspond with excessive growth in your body include insulin, mTOR and IGF-1.
But, to address the problem rather than just the symptom, rather than merely targeting a reduction in these hormones, we need to create an environment where these hormones return to healthy levels.
Insulin
Many people with cancer are insulin resistant. High levels of insulin is typically accompanied by elevated blood sugars (i.e. diabetes or pre-diabetes).
Insulin is a critical hormone in your metabolism. We need some of it to stop our stored energy from being released in an uncontrolled manner into the bloodstream (which occurs in people with Type 1 Diabetes without injected insulin). However, high levels of insulin facilitate excessive levels of growth, particularly in cancer cells that have more insulin receptors.
Insulin helps your cells to grow (i.e. anabolic) as well as to slow their breakdown (i.e. anti-catabolic).
Your body’s repair function (autophagy or self-eating) occurs when insulin levels are low. Hence, it is crucial to reduce your insulin to healthy levels to allow your body’s natural repair and cleaning functions to be activated.
Having a waist to height ratio of greater than 0.5 or a waking blood sugar above 5.6 mmol/L or 100 mg/dL is an indication that your insulin levels are above optimal levels.
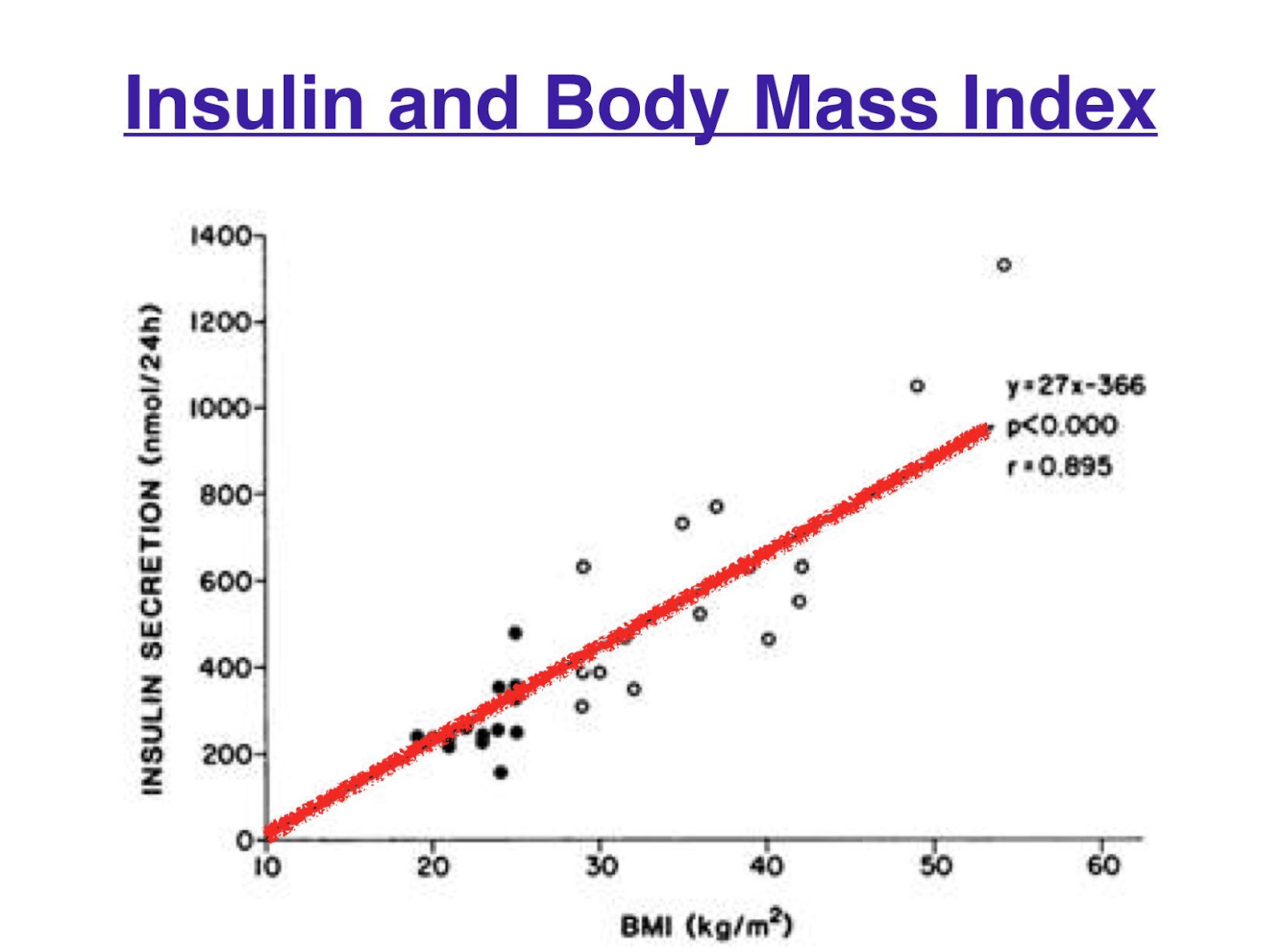
As shown in the chart below, high levels of insulin across the day tend to correlate with a high BMI (i.e. excess stored energy in your body).
While a diet with less processed carbohydrates will enable you to stabilise insulin levels, reducing insulin across the day (not just after meals) requires a reduction in body fat. Once you drop below your Personal Fat Threshold, your body fat stores can absorb energy from your food rather than having it back up into your bloodstream (in the form of elevated blood sugars and free fatty acids).
mTOR
Mammalian Target of Rapamycin (mTOR) is another hormone that your body requires, but in excess, it can be problematic.
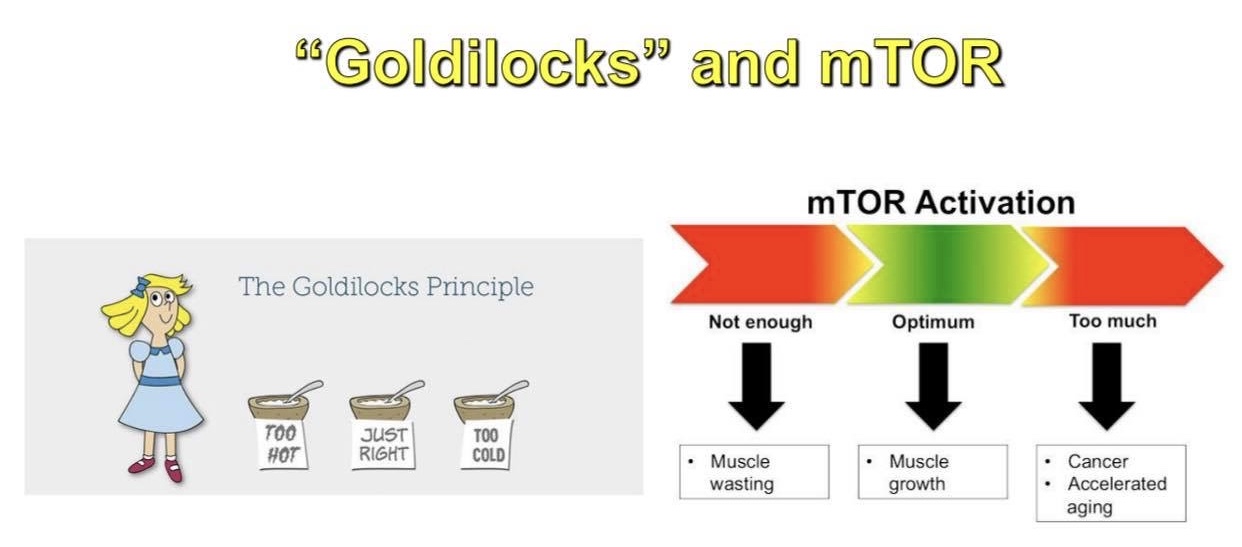
If we don’t have enough mTOR, we can’t grow or build and repair our muscles. We would waste away. But as we get older and no longer need to grow, an environment that promotes continual growth without periods of repair can drive cancer growth.
While protein increases mTOR the most, we also need energy to grow and support all tissues and cells in our body (including our anticancer immune cells). Finding the right balance of a nutrient-dense diet with adequate protein and other nutrients without excessive energy is critical to optimising mTOR.
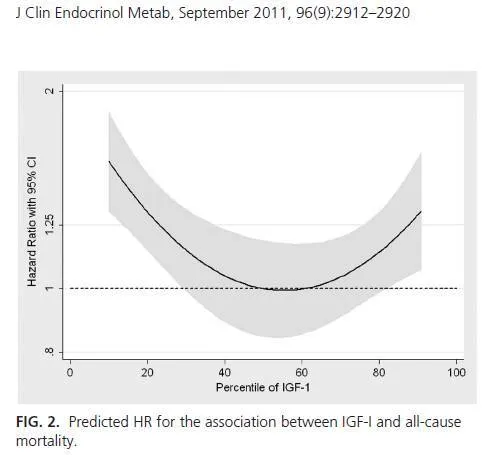
IGF-1
Insulin-Like Growth Factor (IGF-1) is another hormone that aligns with growth, including cancer. As shown in the chart below, our risk of death from any cause increases when we have too little or too much IGF-1.
While protein also stimulates IGF-1 and mTOR, any energy excess that leads to high insulin levels in the body will also stimulate mTOR.
Similar to insulin, the best way to reduce mTOR and IGF-1 to healthy levels is to reduce your overall energy intake levels to reduce body fat. A person with cancer who is carrying excessive levels of body fat needs to find a way of eating that provides nutrients without excessive calories (i.e. a high satiety nutrient-dense diet).
You may be noticing a common theme.
Uncontrolled growth (particularly cancer) occurs in an environment of excess energy. Finding a way of eating that provides greater satiety to enable you to eat less over the long term while still getting the nutrients you need is critical, particularly when it comes to cancer.
Protein
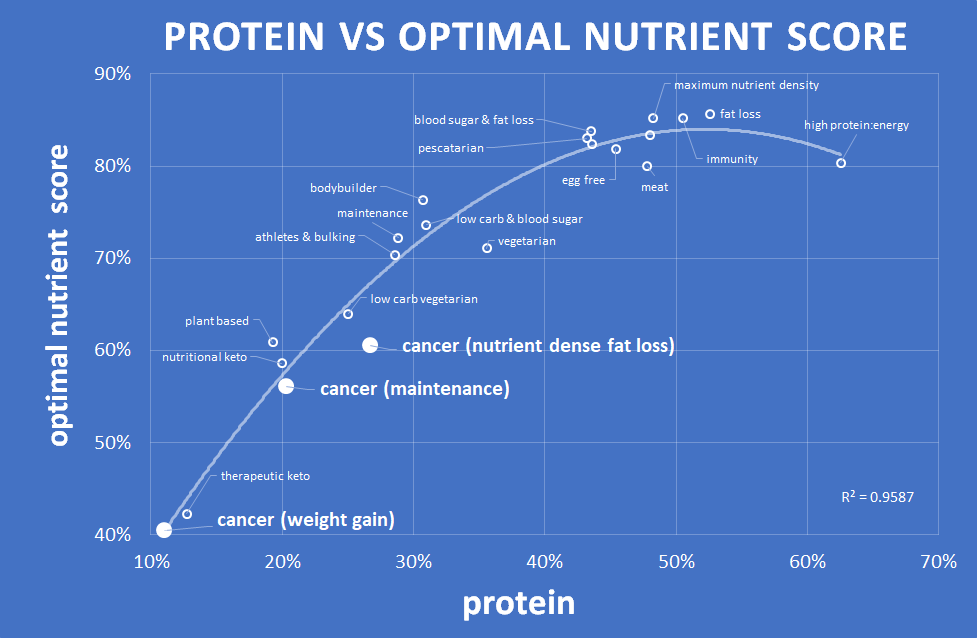
Protein is critical for growth, including cancer. However, effective cancer treatment is not as simple as eliminating all protein. Nutritional optimisation is a balancing act to ensure you get adequate protein. But there is no need to overdo it, particularly if you are managing cancer.
We have found repeatedly through our analysis that a higher percentage of protein in your diet will support greater satiety, which is critical to reducing body fat and bringing your hormones (e.g. insulin, mTOR and IGF-1) down to healthy levels.
The chart below from our analysis of forty thousand days of food diary data from Optimisers shows that as our protein percentage increases, we tend to eat fewer calories.
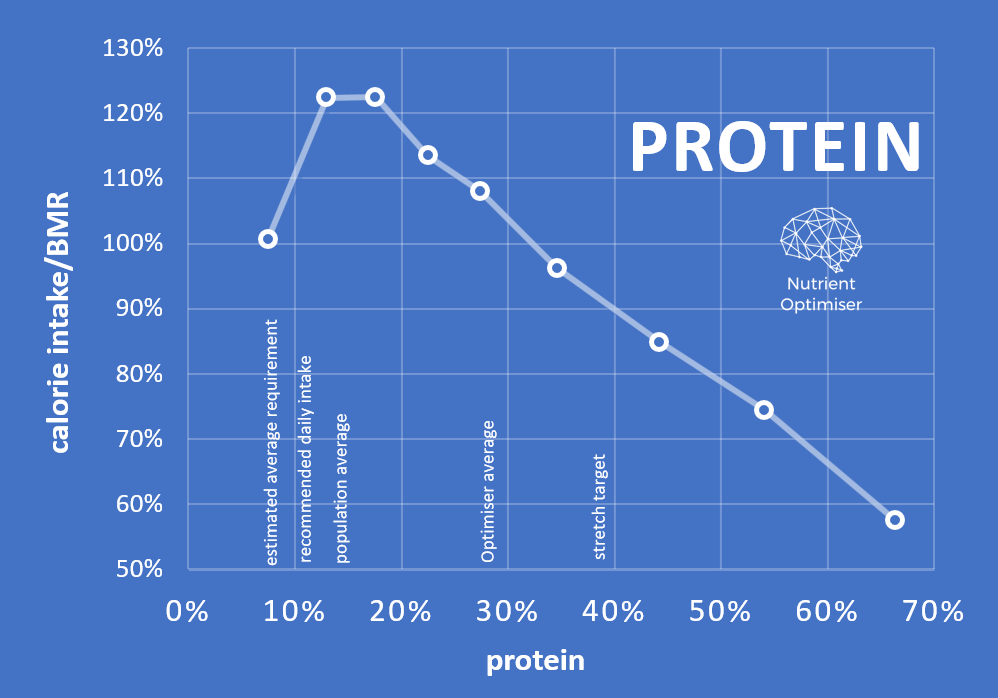
To be clear, this is not merely about eating more protein. More protein (which often comes packaged with fat) tends to align with a greater overall energy intake. As shown in the chart below, if we simply eat more protein, we tend to consume more calories.

Focusing on a higher percentage of protein rather than more protein is a subtle but important distinction.
Your goal should be to get adequate protein to support healthy levels of muscle mass while reducing the easy energy from carbohydrates and fat in your diet. This leads to greater satiety and fat loss over time and hence an environment that is less likely to support cancer growth.
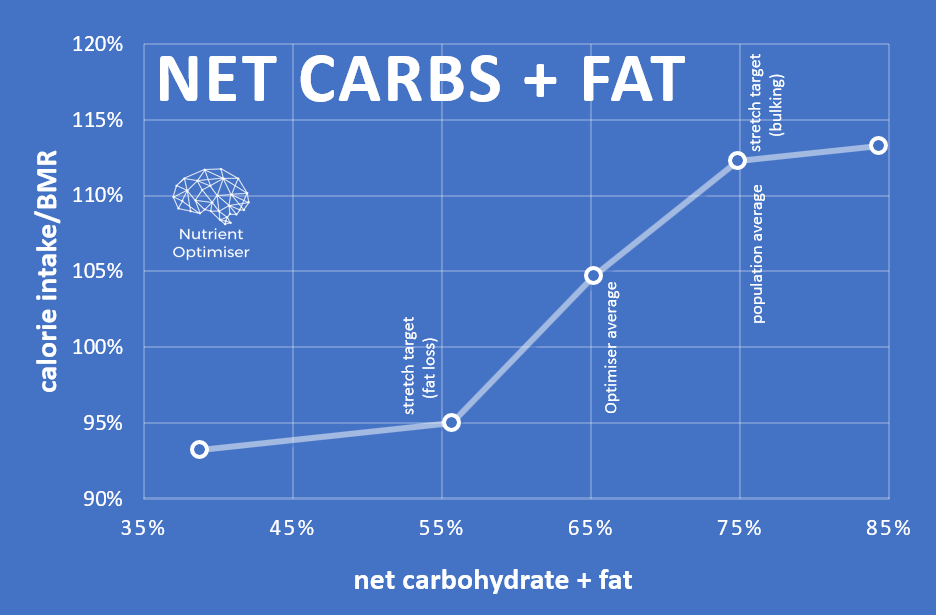
A diet that contains more energy from carbs and fat together (e.g. processed modern junk food) tends to drive us to eat more than we need.
We have continually found that protein is strongly correlated with nutrient density. We can’t simply avoid protein while still nourishing the body with adequate nutrients that it needs to thrive and recover. Adequate protein is also critical to your immune function, therefore critical to cancer recovery.
The chart below from the analysis of our series of 22 recipe books shows that a higher protein percentage tends to align with a more nutritious diet.
The table below shows the protein intake in terms of grams per kilo body weight (BW) and grams per kilo lean body mass (LBM) assuming a 70 kg man with 20% body fat. These values are in line with the generally recommended healthy protein intakes without being excessive.
| nutrient-dense | maintenance | weight gain | |
| % protein | 27% | 20% | 11% |
| baseline calories | 2000 | 2000 | 2000 |
| body fat (%) | 20% | 20% | 20% |
| weight (kg) | 70 | 70 | 70 |
| lean body mass (kg) | 56 | 56 | 56 |
| surplus/deficit (%) | -25% | 0 | 25% |
| actual calories per day | 1500 | 2000 | 2500 |
| protein (g/day) | 101 | 100 | 69 |
| protein (g/kg BW) | 1.4 | 1.4 | 1.0 |
| protein (g/kg LBM) | 1.8 | 1.8 | 1.2 |
From our analysis of forty thousand days of data from Optimisers, we see that as people increase the nutrient density of their diet, they naturally tend to consume fewer calories. Rather than simply trying to restrict your intake, successful long term weight loss requires a shift towards improved diet quality.
Fat and ketones
While cancer cells prefer glucose and low carb or ketogenic diets have been found to help slow cancer growth, cancer cells can also use fat and ketones for fuel to grow.
The chart below (from Ketogenic diet in cancer therapy) shows a review of studies where a low carbohydrate or ketogenic diet is beneficial for a range of different types of cancer.
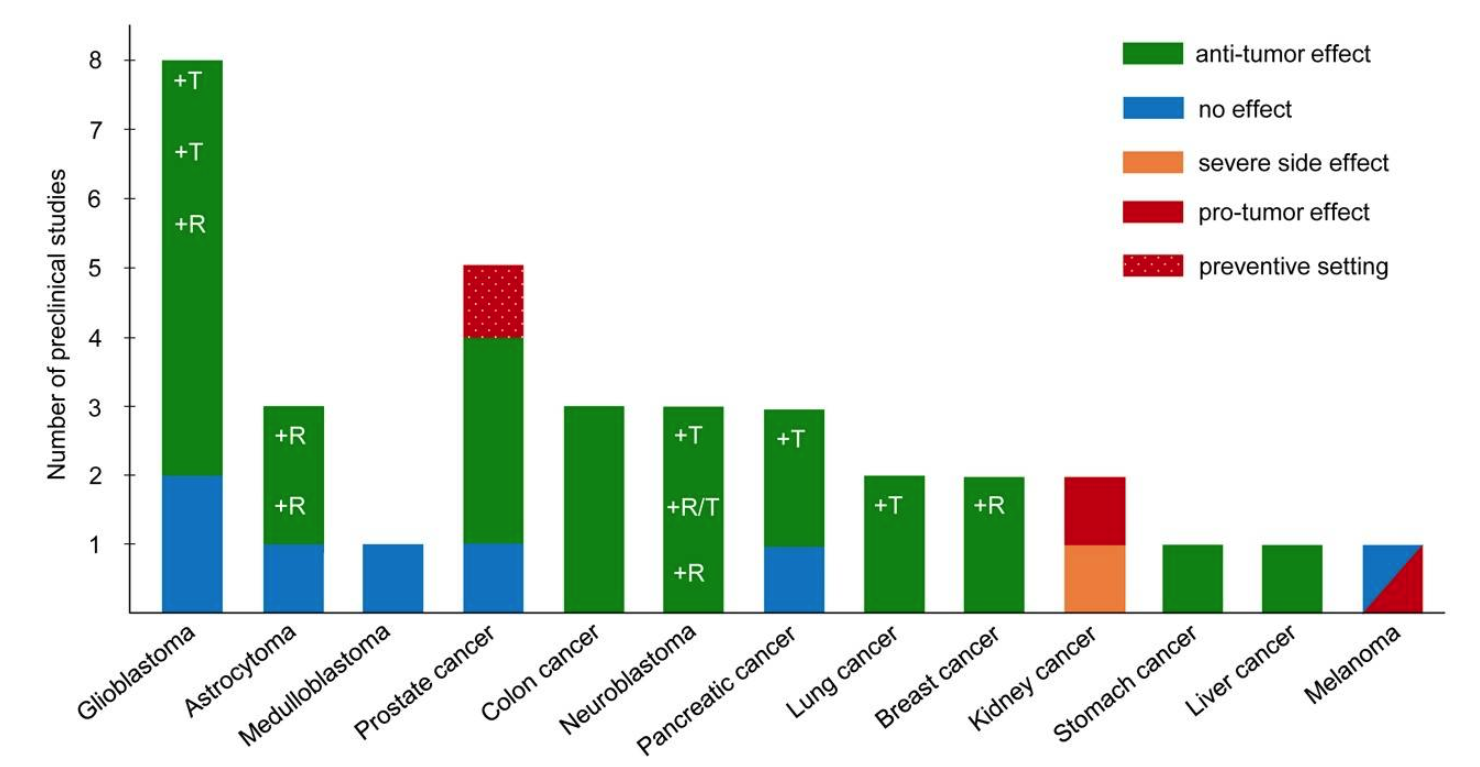
Overall, it appears that a diet with reduced carbs can be a helpful adjunct to cancer therapy. Cancer survivor and friend Andrew Scarborough noted, in reviewing this article, “that there are also many other drugs and other agents that compliment a ketogenic approach nicely, acting on the same pathways and pushing things along further than you could with diet alone.”
However, a high intake of dietary fat can prevent you from using fat from your body which will, in turn, keep your insulin levels high. At the same time, your body needs enough fuel to survive. As shown in the chart below (from the analysis of our series of our recipe books), a lower percentage of dietary fat tends to align with a higher nutrient density.
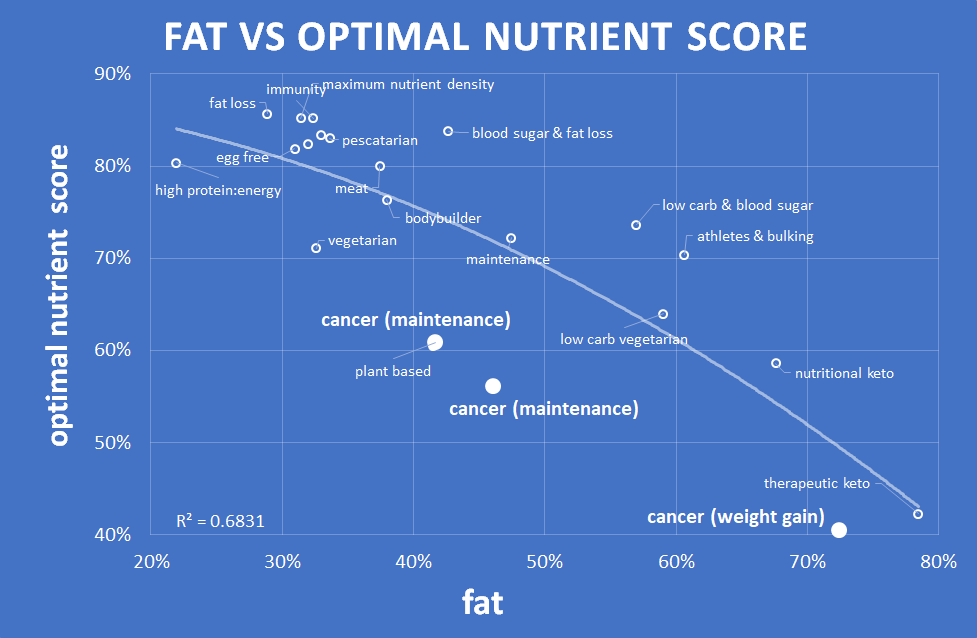
So, while fat can be a useful fuel for someone who needs to gain weight to recover from cancer, if they are obese and trying to lose weight, then we can wind back the dietary fat to promote greater satiety and weight loss, while also providing adequate energy.
Should you go ‘plant-based’ or ‘vegan’ to manage cancer?
Sadly, any discussion about nutrition, including relating to cancer, often goes no further than thinking in terms of macronutrients (i.e. protein, fat and carbs) or plants vs animal foods. People assume that they need to swing to either one extreme or another. But again, optimal rarely lies at the extremes. We need to balance the various factors.
A recent meta-analysis found “the possible absolute effects of red and processed meat consumption on cancer mortality and incidence are very small, and the certainty of the evidence is low to very low.”
Our process of Nutritional Optimisation enables us to move beyond an overly simplistic plants vs animals approach to look at the micronutrients that drive cancer growth and ensure that we achieve an optimal intake of the nutrients that also provide benefit.
Nutrients that affect cancer growth
In addition to MACROnutrients and satiety, some MICROnutrients have been found to fuel excessive cancer growth. We can de-emphasise these when designing a suite of recipes for cancer.
The research in this section has been highly influenced by a March 2020 paper Dietary modifications for cancer therapy by MIT Professor David Sabatini in the prestigious journal Nature. We are incredibly excited to be able to apply Sabatini’s analysis of cancer pathways and mechanisms using nutritional optimisation.
Rather than thinking in terms of individual nutrients or supplements, our database of recipes enables us to use a multicriteria analysis to prioritise recipes that contain specific nutrients in the context of whole foods that, beyond the essential vitamins and minerals, provides a broad range of beneficial compounds.
Glutamine
While glutamine is the most abundant amino acid in the human body, it has also been found to play a key role in cancer metabolism. Cancer cells consume an inordinate amount of glutamine to facilitate their growth, and many modern cancer drugs and treatments intentionally target the action of glutamine to slow cancer growth.
While it is hard to remove glutamine from a nutritious diet, our recipes designed for people managing cancer de-emphasise glutamic acid to reduce one of the primary fuels for cancer growth.
Note: Foods that are highest in glutamic acid include soy products, shrimp, and beef.
Methionine
Methionine is another amino acid that is critical for cancer growth, particularly in tumours. Dietary restriction of methionine has been shown to enhance cancer treatment in mouse models for a range of cancer types, including carcinoma, glioma, prostate cancer, colorectal cancer, breast cancer and melanoma.
It is also challenging to eliminate methionine from a nutritious diet. However, we have designed the cancer recipe books to de-emphasise methionine to prioritise recipes that contain less methionine.
Foods that are highest in methionine include eggs, shrimp/prawns and some fish.
Serine
Serine is another amino acid that cancer cells require to support their proliferation. Cancer research indicates that dietary restriction of serine has the potential to slow tumour growth. The restriction of serine in the diet also enhances the action of metformin which is sometimes used in cancer therapy.
Hence, our cancer management recipes de-emphasise serine.
Foods that contain more serine include egg whites, soy protein, cheese and some seafood products.
Aspartate
Low levels of aspartate, the amino acid which is required for protein synthesis, can be growth limiting under hypoxic conditions, which are common in tumours. Hence, our cancer management recipes de-emphasise aspartate.
Foods that contain more aspartate include soy protein, shrimp and asparagus.
Histidine
The drug methotrexate was one of the first approved anticancer drugs and is a cornerstone of modern chemotherapy treatment. However, this therapy can cause toxicity as it depletes histidine to dangerous levels for the person undergoing the treatment.
However, it has recently been found that increasing the dietary intake of the amino acid histidine can increase the sensitivity of cancer cells to methotrexate and lower the negative side effects of methotrexate treatment. Our recipes designed for cancer emphasise recipes that contain more of the amino acid histidine.
Foods that contain more histidine include game meats, pork and beef.
Folate
Folate (vitamin B9) is a nutrient that is critical for growth, including tumour cells. The antifolate drug methotrexate is the standard of care for leukemia to target the synthesis of nucleotides that are in high demand for fast-proliferating cancer cells. Hence, our cancer management recipes de-emphasise folate.
Foods that contain more folate include yeast extract, spinach, asparagus and turnips.
Vitamin B12
Similar to folate, vitamin B12 tends to promote growth, and excessive supplementation has been shown to increase the risk of lung cancer. Hence, we have chosen not to emphasise vitamin B12 in the recipes to avoid excessive levels of vitamin B12.
Reduce not eliminate
To summarise, in line with the latest research into cancer metabolism, to optimise food choices for people managing cancer, we want to limit glutamine, methionine, serine, folate and aspartate while providing more histidine. It’s important to note that we are not eliminating these nutrients, but rather, reducing them.
The micronutrient fingerprint shows the resultant nutritional profile when we apply this approach. You can see we get a low protein outcome (i.e. 11% protein) with less of most of the amino acids. Fat is relatively high (71%), and non-fibre carbohydrates are relatively low (15%).
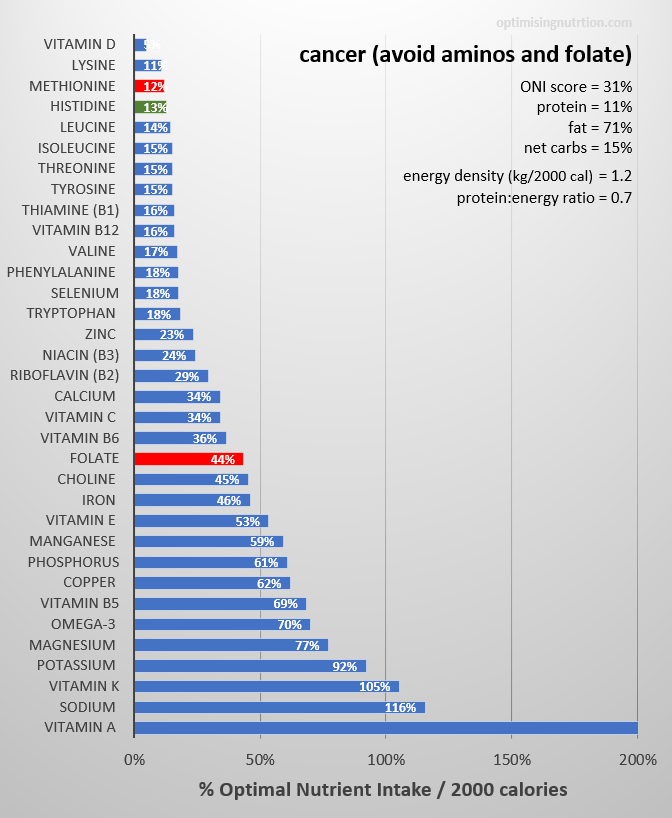
The problem is that the overall outcome is not particularly nutrient-dense, particularly when compared to the approaches that focus on more vitamins and minerals.
In the following section, we will look at how we can remedy this by adding in more of the vitamins and minerals that tend to be harder to find when we avoid protein.
Nutrient density and cancer
While limiting some specific amino acids appears to be beneficial for cancer management, we believe that nutrition should be primarily about prioritising the nutrients that you require to thrive. Once you give your body the things it needs, it has a better chance of being able to repair naturally.
The essential nutrients (i.e. vitamins, minerals, essential fatty acids and amino acids) are the building blocks and co-factors that your body needs to fight cancer and recover from treatments. As we accumulate nutrient deficiencies, systemic inflammation and oxidative stress levels increase and are associated with worse cancer and overall health outcomes:
- impaired immune function,
- mitochondrial dysfunction (decreased cellular energy production, increased oxidative stress and inflammation, aging),
- impaired methylation (involved in gene activation/deactivation, DNA protection, detoxification, etc.),
- insulin resistance,
- increased risk of cardiovascular disease events,
- gut dysbiosis, inflammation, leaky gut,
- mood, cognitive and memory issues,
- endocrine imbalance (stress hormones, sex hormones, thyroid hormonal abnormalities, etc.),
- impaired detoxification pathways, and
- appetite stimulation & weight gain.
As noted in the study Micronutrients and Cancer, poor nutrition and the overconsumption of energy seem to play a significant role in cancer.
Through the research work of David Sabatini and others, we have a good understanding of how amino acids affect cancer. However, it is not as clear which vitamins and minerals are beneficial (particularly when it comes to supplements).
Note: Before you go out and buy a big bag of supplements to optimise your cancer therapy, you should be aware that isolated micronutrients supplements can worsen your cancer risk by overdriving some functions in your body and creating imbalances. You should check with your medical team before relying on supplements for your micronutrient intake as they can impair the effectiveness of cancer treatment. While there may be a role for supplements if you are unable to eat whole foods (e.g. if you are relying on a feeding tube to eat), supplements are no substitute for nutrient-dense whole foods.
While researchers are yet to isolate which specific compounds and nutrients in foods provide the benefit, there is no argument that a nutritious whole food diet is beneficial when it comes to cancer.
People who have cancer tend to have a poorer nutritional status than healthy people. A robust nutritional status is critical to our immune system and healing process. It appears that people recovering from cancer may need a lot more nutrients in their diet than the general population.
Hence, in addition to de-emphasising particular amino acids, our suite of nutrient-dense recipes optimised for cancer also boost vitamin D, vitamin B1, niacin, zinc, selenium, calcium and vitamin C.
While doing this will increase the protein percentage, we achieve a much more nutrient-dense and satiating dietary outcome. Greater satiety means that someone trying to lose weight will be able to eat less with less hunger while still getting adequate vitamins and minerals and sufficient (but not too much) protein.
Do you still need to use supplements?
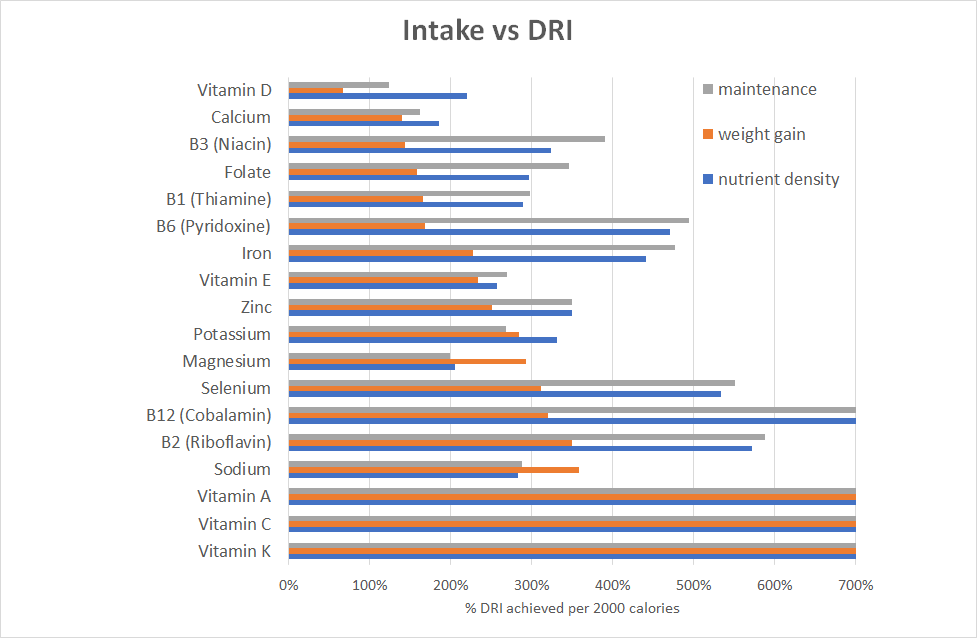
One common question in the development of these recipe books was whether someone using these recipes would still need to supplement. There may be benefits in supplementing to achieve the Dietary Reference Intakes (DRI) if these minimum requirements cannot be met by food alone, however, supplementing above these levels may be unnecessary and potentially risky.
The nutrient fingerprint charts in this article show the intake in terms of Optimal Nutrient Intake, which is typically much higher than the Dietary Reference Intakes which are simply designed to prevent diseases of deficiency in the majority of the population (i.e. not optimal health or satiety). To understand how the different recipe books compare with the DRI, we prepared the charts below which show the essential vitamins and minerals in terms of nutrients provided per 2000 calories. Overall, we can see that these recipes provide significantly more than the DRI for all but vitamin D in the weight gain approach.
However, we also need to consider that each of the approaches is designed intentionally to drive a higher energy intake (in the case of weight gain) and a lower energy intake (in the case of the maximum nutrient density recipes. To correct for this, we have adjusted the nutrient intakes, with a 30% deficit for the maximum nutrient density recipes and a 30% calorie excess for the weight gain recipes.
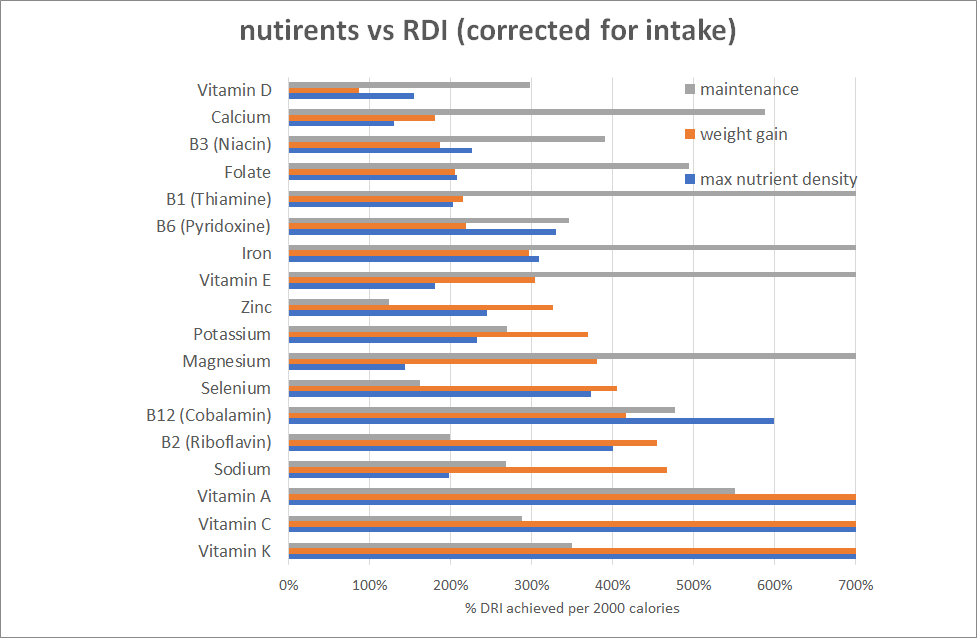
When corrected, we see that we can achieve several times the minimum nutrient intakes to prevent deficiency. Hence, you will be able to save your money on the supplements to invest in nutrient-dense whole food.
Note: It is difficult to obtain the DRI for vitamin D from food alone. The target intake levels are based on the assumption that you will produce some vitamin D from regular sun exposure. Hence, Vitamin D is the one nutrient you may need to consider supplementing if you are unable to get significant sun exposure.
What about the various cancer phenotypes?
Again, cancer is complex. Different types of cancers can benefit from the inclusion of different nutrients. Some of these you can get from your food while some you may need to supplement. However, again, we recommend you work with your medical team to identify if any of these supplements would positively or negatively affect your specific type of cancer and treatment.
We have spent some time looking at how the different nutrients would change the nutritional recommendation and found that the base recommendations for cancer are most useful. From there, you can look to overlay specific drugs or targetted supplements that may be beneficial.
Weight gain
So far, we’ve talked about the approaches to maximise nutrients while also maximising satiety for weight loss and insulin resistance. But there are other people with cancer who need to gain weight.
Unfortunately, many people lose their appetite when going through cancer and hence lose a lot of weight, including precious muscle mass. Regaining strength and body weight with enough energy to support healing and recovery is critical for these people.
Sadly, many of the meal replacement products provide very little in the way of nutrition (i.e. other than synthetic supplements which, as noted earlier, don’t tend to provide the same benefit).
Hence, we also created a suite of recipes that contain plenty of energy to support weight gain after cancer treatment.
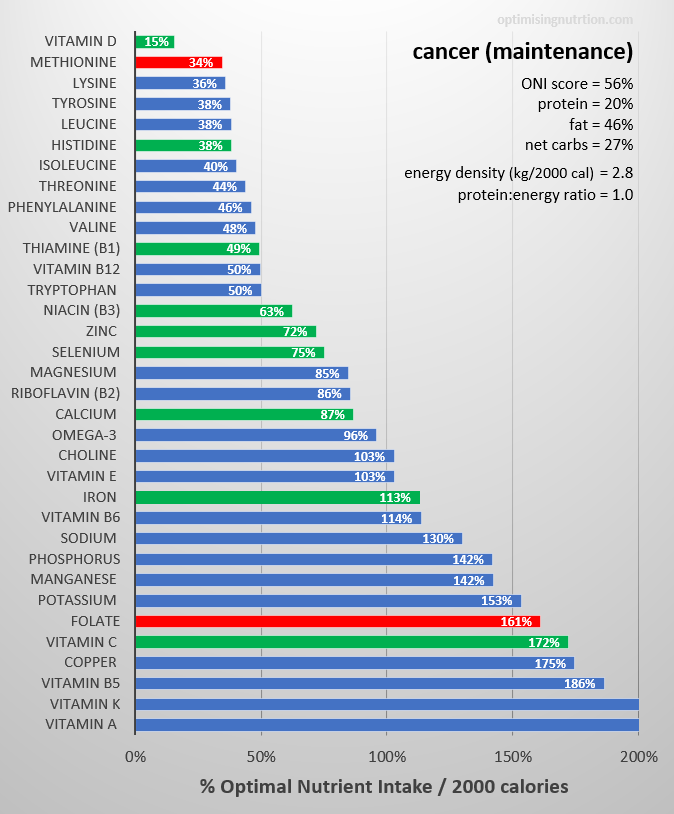
The nutrient fingerprint chart below shows the nutrients that these recipes contain. These meals have a higher energy density and a lower protein:energy ratio which will allow people to consume more of them while still providing a significant amount of nutrients (though not as much as the nutrient-dense option).
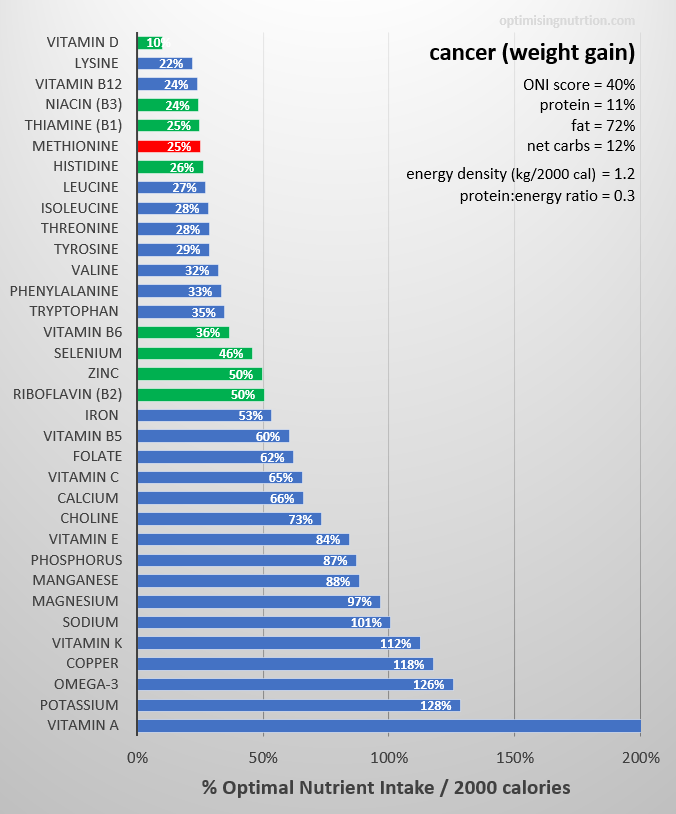
These recipes are ideal for someone with cancer while providing plenty of energy to support weight gain during and after cancer treatment. Some examples of the highest-ranking recipes for people with cancer who need to gain weight are shown below.







Weight maintenance
Finally, we come to the weight maintenance option.
This suite of recipes has been designed to provide enough energy to maintain a healthy weight. They may be one of the few who made it through cancer treatment without suffering weight loss, or perhaps they have regained some weight after cancer treatment and are ready to get on with weight maintenance while still keeping an eye on their cancer risk.
The chart below shows the nutrient fingerprint for this suite of recipes. As you can see from the earlier charts, they sit between nutrient-dense and weight gain approaches.
Some examples of nutrient-dense recipes that rank well for people with cancer trying to maintain their weight are shown below.




Summary
At its essence, cancer is the excessive and continued growth of defective cells. Obesity, caused by a constant flow of excessive energy, fuels cancer growth. Hence, the first step in avoiding and starving cancer is to create a lower energy environment. This can be achieved by prioritising high satiety nutrient-dense foods and meals to achieve a more ideal body composition, thus reducing growth-related hormones (e.g. insulin, IGF-1, mTOR, etc.).
Recent research has found that specific nutrients in our food tend to promote cancer growth more than others (e.g. simple carbohydrates, glutamine, methionine, serine, folate and aspartate). While we can identify foods and meals that contain less of these cancer-promoting nutrients, the resultant foods tend to be nutrient-poor overall.
While supplements tend not to be useful, it is clear that people diagnosed with cancer tend to have a poor nutrient status and they also require more nutrients than to recover from cancer and the associated treatments effectively. To address this, we also emphasise other nutrients that are harder to find in a low protein diet.
Although many people are obese when they find they have cancer, aggressive treatments such as chemotherapy and some drug treatments tend to cause wasting and lack of appetite. To address this, we have created a suite of recipes optimised for people with cancer to enable them to:
- lose weight before cancer treatment (i.e. high satiety nutrient-dense),
- gain weight after cancer treatment (i.e. energy-dense, low satiety), and
- maintain weight once they have achieved a healthy weight.
The recipe books
If you’re interested in trying these recipes designed for the unique needs of people managing cancer, you can purchase them here.
What do you get?
- An ebook with 33 of the most nutritious meals optimised for cancer (that you can take with you anywhere on your phone or tablet).
- A secret index of links to the 150 most nutrient-dense recipes on our website so you will never run out of nutritious ideas to try.
- A full micronutrient breakdown showing the vitamins, minerals, essential fatty acids and amino acids that you will obtain from every recipe.
- Access to all the recipes pre-logged in Cronometer for your convenience.
- A list of the most popular nutrient-dense foods optimised for people managing cancer.
Now that you’ve taken a deep dive into the cancer lake, how about tackling the histamine-intolerant one? You will find in your journey that both histamine intolerance and cancer have a link–mast cell cancer. I want to see you create a histamine intolerance book of recipes, since a lot of traditional, keto go-to’s are now off limits, and proper nutrient density gets real hard at this point.
This is excellent! Highly recommended!
Wow! Thank you! Really glad you liked it!